The Endocannabinoid System and Sleep
The ECS is a signaling system in the brain and body that helps regulate your internal balance—including sleep cycles, circadian rhythms (your body’s internal 24-hour clock), and energy. It has three main parts:
- Your body’s own cannabinoids—primarily anandamide and 2-arachidonoylglycerol (2-AG)
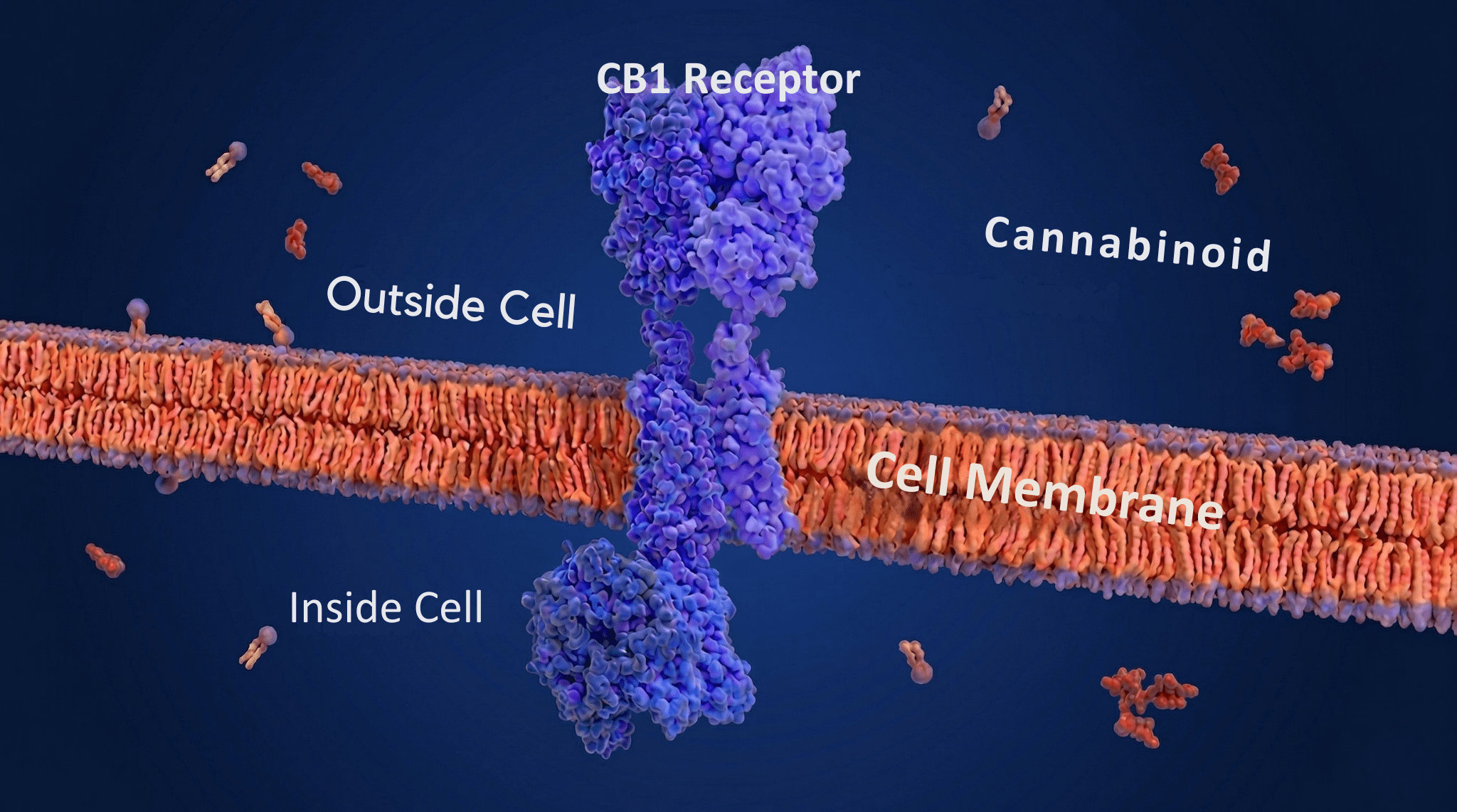
- Cannabinoid receptors, mainly CB1 and CB2, found throughout the brain and body
- Enzymes that build and break down those cannabinoids (Mechoulam & Parker, 2013)
CB1 Receptors and Sleep
CB1 receptors are spread throughout the brain areas that control sleep—including the hypothalamus, basal forebrain, and brainstem (Lutz et al., 2015). They regulate the release of chemical messengers, particularly GABA (which slows brain activity) and glutamate (which excites it), directly affecting how awake or drowsy you feel (Murillo-Rodríguez et al., 2008). In animal studies, activating CB1 receptors increased NREM sleep—the deep, dreamless stages—and shortened the time needed to fall asleep, findings that have been partially confirmed in human studies using THC (Pava et al., 2016; Nicholson et al., 2004).
When researchers blocked these same CB1 receptors in animal studies, sleep became fragmented and dream sleep shortened—showing that these receptors work in both directions, either promoting or disrupting healthy sleep depending on whether they’re activated or blocked (Pava et al., 2016).
Using THC regularly over time causes the brain to dial back its CB1 receptors—reducing their number and making them less sensitive to stimulation. This is why tolerance develops: you need more THC to get the same effect, and over time, sleep quality can actually worsen as a result (Lutz et al., 2015).
Daily ECS Rhythms
The ECS follows its own daily rhythm. Anandamide levels tend to rise during the early morning hours—the time humans are typically asleep—suggesting it plays a role in helping sleep begin (Murillo-Rodríguez et al., 2006). 2-AG levels peak later in the day, potentially supporting wakefulness and energy balance (Vaughn et al., 2010).
How CBD Works Differently
CBD doesn’t bind strongly to CB1 or CB2 receptors. Instead, it targets receptors involved in mood, pain, and relaxation—including serotonin receptors, TRPV1 channels, and adenosine receptors—in ways that promote calm and may indirectly support sleep, especially in people whose insomnia is driven by anxiety (Russo, 2011; Shannon et al., 2019).
The relationship between sleep and the ECS runs both ways. Disrupted sleep can also throw the ECS off balance—and altered ECS function has been found in people with chronic insomnia, sleep apnea (a condition where breathing repeatedly stops during sleep), and PTSD. This suggests cannabis-based therapies might work by targeting the brain processes already involved in these conditions (Babson et al., 2017).
What THC, CBD, and CBN Do to Your Sleep
THC: Faster to Sleep, Less Dreaming
Sleep moves through two main stages: NREM sleep—the deep, restorative phases—and REM sleep, the stage when you dream, store memories, and process emotions (Carskadon & Dement, 2011).
THC shortens how long it takes to fall asleep but also consistently reduces time spent in REM sleep (Cousens & DiMascio, 1973; Schierenbeck et al., 2008). For people with PTSD, that reduction in dream sleep can mean fewer nightmares (Fraser, 2009). But over time, suppressing REM may impair memory and emotional regulation (Walker, 2009).
CBD: A Two-Phase Effect
CBD behaves differently depending on the dose—small amounts can be alerting, while larger amounts tend to be sedating. In animal studies, low-to-moderate doses activated brain systems involved in wakefulness, suggesting potential for treating daytime sleepiness, though human trial evidence for this remains limited (Murillo-Rodríguez et al., 2008; Chagas et al., 2014).
At higher doses, CBD has been shown to increase total sleep time and deepen sleep in human case series (detailed reports on results from a group of real patients) (Shannon et al., 2019). In practical terms: lower doses earlier in the day may help you stay alert, while higher doses in the evening may help you sleep.
CBN and the Entourage Effect
CBN—a compound produced as THC breaks down over time—has attracted interest as a sleep aid. Early research and anecdotal reports suggest it may extend total sleep time without suppressing dream sleep. But rigorous human studies are limited, and because CBN is almost always consumed alongside leftover THC and other cannabinoids, figuring out what CBN does on its own is genuinely difficult (Russo, 2011).
This gets into what’s called the entourage effect—the idea that cannabinoids, terpenes, and other plant compounds work better together than any one of them does alone. Myrcene may boost the sleep-promoting properties of THC or CBN (Russo, 2011), while linalool has shown sedating effects in animal studies (Linck et al., 2009). A well-matched ratio of THC and CBD with the right terpenes may offer better results than any single compound alone.
Cannabis and REM Sleep
Reducing REM sleep is one of the most consistent effects of cannabis documented in research. Studies going back to the 1970s found that moderate-to-high THC doses cut the proportion of time spent in dream sleep while increasing slow-wave (deep) sleep (Cousens & DiMascio, 1973; Feinberg et al., 1975).
This happens because THC activates CB1 receptors in the brainstem—the part of the brain that controls wakefulness and triggers dream sleep. That activation disrupts the brain chemicals that normally switch REM sleep on, including serotonin and norepinephrine (two chemicals that regulate mood and arousal), delaying REM and cutting it short (Murillo-Rodríguez et al., 2008).
The relationship runs both ways. When people who use cannabis nightly reduce or stop, many experience a REM rebound—a temporary surge of intense, vivid dreaming that can be jarring (Feinberg et al., 1976; Schierenbeck et al., 2008). CBD, by contrast, may modestly increase REM sleep at moderate doses through its anti-anxiety and serotonin-related effects (Babson et al., 2017). How much any of this matters in practice depends on the cannabinoid mix, dose, product type, and how often someone uses (Babson et al., 2017; Suraev et al., 2020).
Cannabis and Your Body Clock
The ECS follows its own daily rhythm: anandamide and 2-AG levels rise and fall throughout the day in sync with waking, eating, and sleep (Valenti et al., 2004; Murillo-Rodríguez et al., 2006). When THC or CBD is introduced, it can shift these rhythms by changing how active the ECS is at different points in the day.
Timing matters. High-THC cannabis used late in the evening may help you fall asleep faster (Nicholson et al., 2004). High-CBD products used earlier in the day may reduce anxiety and nervous system over-activity in ways that could support a more stable sleep-wake cycle—though this comes from CBD’s documented anti-anxiety effects (Shannon et al., 2019) rather than from dedicated circadian studies.
For people with a disrupted body clock—from shift work or jet lag—cannabis might work alongside behavioral strategies. Animal studies show that activating cannabinoid receptors can influence how the brain adjusts to changes in light and darkness, possibly through the suprachiasmatic nucleus (SCN)—the brain’s master clock, located in the hypothalamus (Acuna-Goycolea et al., 2010). The same product may hit differently depending on whether you use it in the morning, afternoon, or evening, which suggests that timing is a real variable that hasn’t been studied enough. Heavy or long-term THC use at night may reduce deep sleep quality and leave you groggy the next day (Feinberg et al., 1975; Schierenbeck et al., 2008). For regular users, strain, dose, and timing all deserve deliberate thought.
Cannabis Tolerance, Withdrawal, and Sleep Disruption
Short-term cannabis use often helps with sleep onset. But long-term use leads to tolerance and, in many cases, rebound insomnia—a temporary worsening of sleep when you stop. Over time, the brain adapts to regular THC by reducing the sensitivity of its CB1 receptors, meaning you need more to get the same effect, and sleep quality can actually decline in the process (Lutz et al., 2015).
When long-term users stop abruptly, withdrawal commonly includes vivid dreams, difficulty falling asleep, and frequent waking. This happens because the brain overcorrects—the chemical systems that THC had been holding in check, including serotonin and norepinephrine signals, fire more strongly than usual. REM sleep, which had been suppressed, comes rushing back, often as intense or unsettling dreams. These disturbances can last several weeks (Budney et al., 2004). Tapering down gradually is a better approach than quitting suddenly.
CBD, which is generally not habit-forming, may ease some withdrawal-related sleep problems through its calming and balance-restoring effects—though the research is still limited and results are mixed.